Agentic AI for Clinics and Hospitals
Vishal Sachar
Co-Founder & CEO of CLRT
Healthcare is widely seen as cautious about AI, and people read that caution as the reason the sector is behind. The real reason is a category error. Caution about clinical decisions is correct and should be absolute. The mistake is extending that same clinical-grade caution to scheduling, paperwork, and documentation, which freezes the safe, valuable work alongside the dangerous kind.
Start with where the value actually is, because the fantasy and the value point in opposite directions. The fantasy is AI that diagnoses, the glamorous, heavily regulated, liability-laden frontier. The value, available now and almost unglamorous, is the recovery of clinician time from the administrative crush that is a leading driver of burnout and the quiet thief of attention that should be on patients.
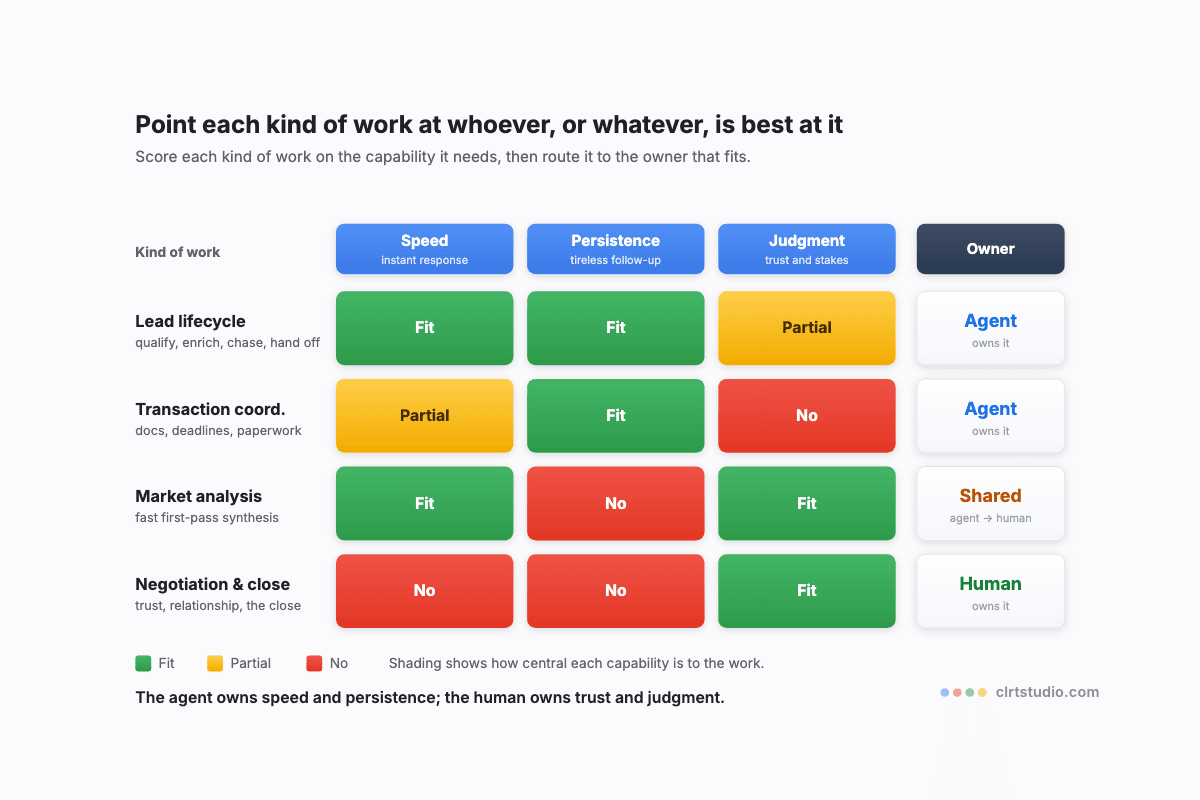
Once you draw the bright line, the agenda organises itself. On the clinical side, the line is firm: AI may assist, surface, and summarise, but a clinician decides, every time, with no exception, because here the model's habit of being confidently wrong is not an inconvenience, it is a patient-safety event. On the administrative side, the brakes can come off: appointment scheduling, patient communication and reminders, prior authorisation, coding support, insurance documentation, and clinical-note drafting that a clinician reviews and signs are mostly the verifiable, rules-and-extraction job-shapes that automate well and pay back fast.
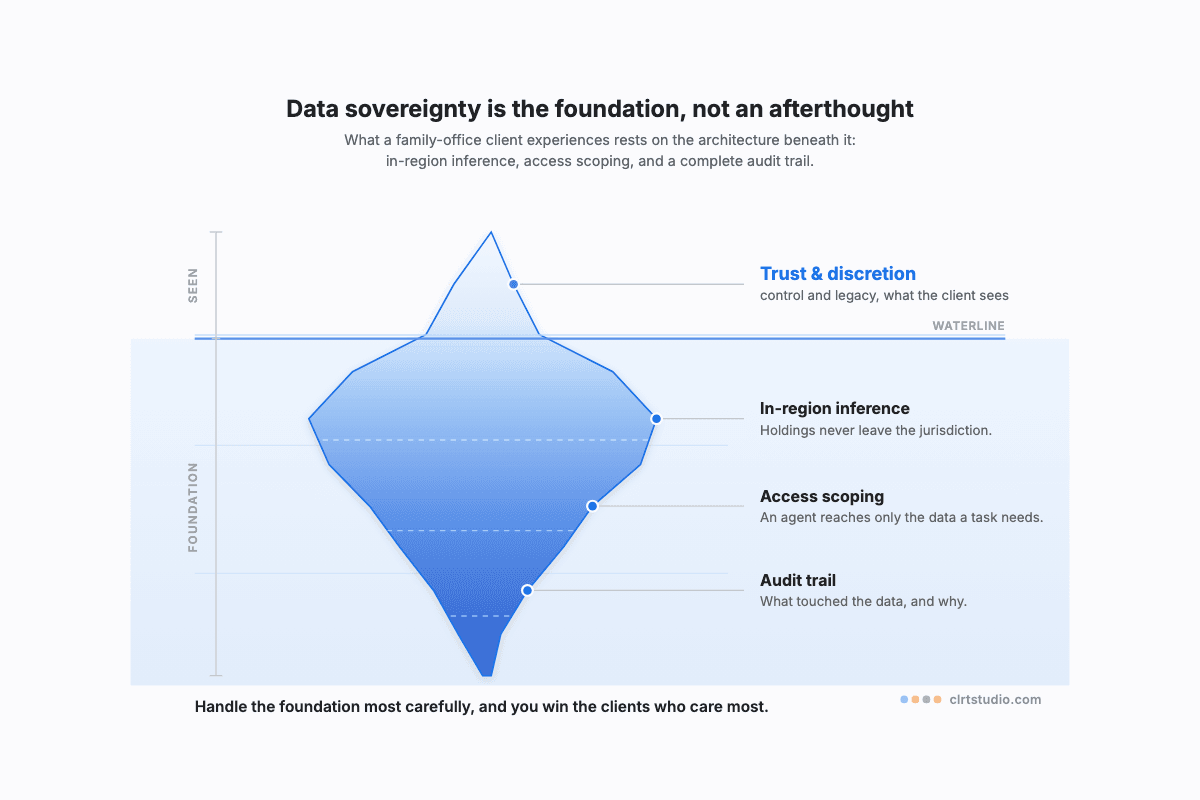
And one constraint sits above all of it. Patient data is the most sensitive category there is, which makes where it is processed a first-order design decision rather than an afterthought, and turns careful handling into both a duty and an advantage, the argument in The Constraint That Is Also a Moat.
Keep the clinical judgment entirely human, automate the clerical burden without apology, and you give your clinicians back the one thing the system keeps taking: time with the patient.
A deeper dive
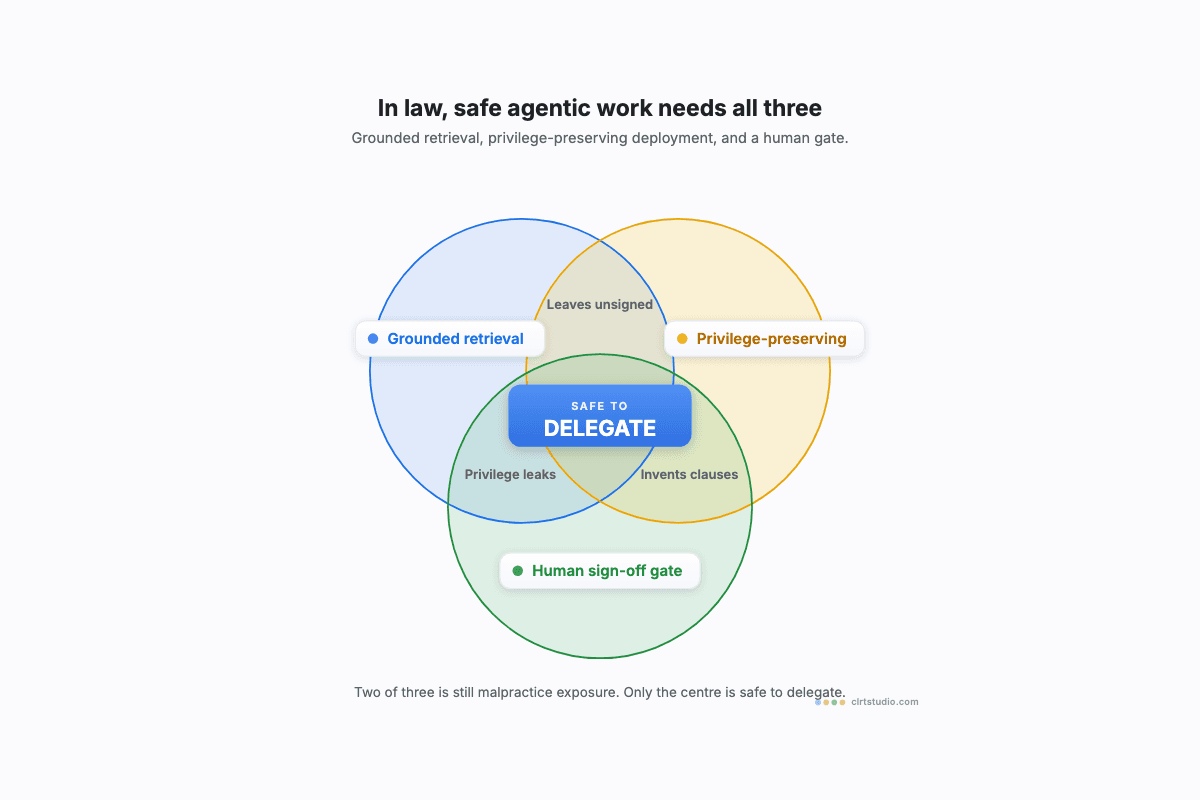
The architecture for anything touching care follows one rule: AI suggests, the clinician decides, and the system is built so that order cannot be reversed. Ambient documentation, where an agent drafts the clinical note from a visit, is the clearest near-term win, but its output is a draft the clinician verifies and signs, never a record that stands on its own, because an unreviewed clinical summary that drops or invents a detail is exactly the invisible, fluent failure that does damage, the argument in Where AI Almost Works Is Where It Hurts You. Prior authorisation and coding are extraction-and-rules jobs that check against a source, so they automate with confidence and a light audit. The data architecture has to treat patient information at the highest residency tier, in-region or dedicated processing, strict access scoping so an agent reaches only what a task requires, and a complete audit trail of what touched a record and why. The deeper point is that in healthcare the verification layer is not a feature you add for safety. On the clinical side it is the practice of medicine, and the agent simply does the assembling beneath a human who remains fully and visibly in charge.
Work with CLRT
The safe, valuable path in healthcare AI opens the moment you stop treating paperwork like surgery. CLRT helps clinics and hospitals automate the administrative burden, with patient-data protection built in, while every clinical decision stays firmly with the clinician. Let us help you draw that line.

Vishal Sachar
Vishal Sachar is the Co-Founder and CEO of CLRT, where he helps UAE businesses make sense of applied agentic AI and put it to work. He writes on agentic systems, AI governance, and the economics of automation. Reach him at vishal@clrtstudio.com or on LinkedIn.